Engagement with Deaf, Deaf-Blind and Hard of Hearing Stakeholders during the Time of COVID-19
by Emina Dervisevic, Director, Engagement + Communications
As you all might have guessed, the global pandemic has affected the world of engagement. We are in the business of getting people together and receiving their input, and the social distancing measures in place in British Columbia, across Canada and around the world have had an impact on us. We have either had to pivot and move our work online, or delay projects for the time being, or accept that some of our projects have been cancelled with the possibility of them never being resurrected.
Despite the growing popularity of Sign language interpreting with Dr. Henry’s daily updates, engaging with “seldom-heard populations”, including Deaf, Deaf-Blind and hard of hearing communities would be one of the first areas to be affected considering that seldom-heard populations could be hard to reach at the best of times. Or so you would think…
Delaney has been involved in the engagement with Deaf, Deaf-Blind and hard of hearing British Columbians since 2017, for a project with the Provincial Language Service (PLS) – an agency of the Provincial Health Services Authority (PHSA). The direct result of the engagement has been the creation of a Community Advisory Group (CAG) consisting of Deaf, Deaf-Blind and hard of hearing community members from across the province who have been selected to advise PLS on the re-design of the Provincial Medical Sign Language Interpreting Services (access to Sign interpreting for medical appointments).
Many Deaf, Deaf-Blind and hard of hearing British Columbians rely on medical interpreters for access to accurate information during their medical appointments and medical treatment, and efficient and effective interpreting service is the first step in assuring they receive proper care. In addition to this, for many British Columbians who have been Deaf since birth, English is not their first language; American Sign Language (ASL) is. The importance of this project and the need to ensure the service re-design continues – despite the pandemic-related challenges – cannot be overstated.
Contrary to the popular belief, the meetings with the CAG didn’t skip a beat. CAG had its third meeting on January 31, fourth on March 20, and fifth just a week ago – on May 4. COVID-19 came, social distancing measures were put in place, lots of work stopped, yet engagement with the Deaf, Deaf-Blind and hard of hearing Community Advisory Group continued. How is this possible?
Here is how we made it happen:
- Deaf communities are technologically savvy. I realized this a couple of years ago in Phase 3 of the PLS engagement. We had 22 Deaf, Deaf-Blind and hard of hearing participants attending in person and calling in via Telehealth. We realized very quickly that the technology piece would be a challenge for all of us hearing people in the room! The participants figured out very quickly how to use the technology and knew exactly what to do.
Once the CAG was set up, as some participants were joining the meetings in person and others were calling in from various parts of BC, we had to test and trial several platforms used by PHSA. We had to think about “angles” to make sure that interpreters were visible. For a while, we were even thinking it would be practical for each person to come with their own device so that they could have their own camera and window. For signing, it is important to clearly see the person’s hands. So, once we were no longer allowed to meet in person, adding a few more people to our virtual calls seemed like a logical next step and not an insurmountable task (which was the case with many of our other projects).
- PHSA quickly approved the use of Zoom. The first time I heard about Zoom it was in one of our engagement sessions (in Prince George, I believe) with Deaf and Deaf-Blind stakeholders, and years before Covid-19. They strongly recommended it because it was user-friendly, it didn’t freeze, and there were different views. The inexperienced me thought that it couldn’t be much different from other platforms – PHSA’s Telehealth, Google Hangout or MS Teams. We ran several of our other meetings on other platforms, but thankfully, PHSA has approved Zoom, and our last meeting was run on Zoom. After this last experience, we are not going back. My only regret is that we didn’t introduce Zoom earlier into the process.
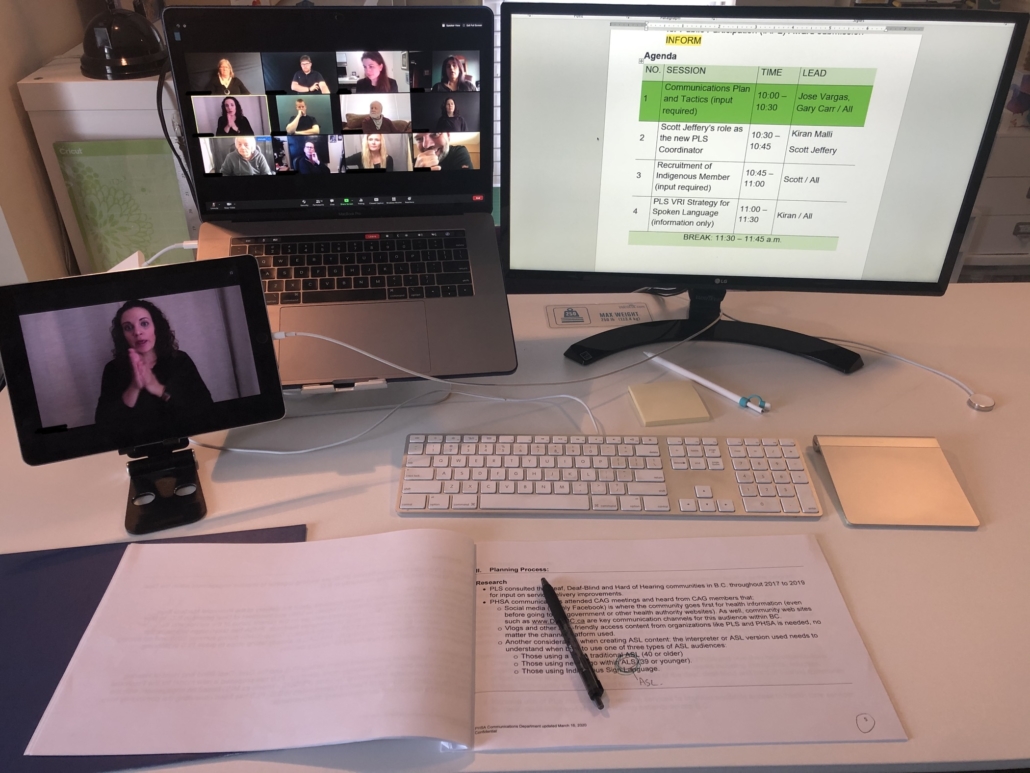
- Interpreting for the Deaf-Blind participant needed special arrangements. Since we moved the meetings online, the meetings have been the most challenging for the Deaf-Blind participant. He was unable to determine who was signing in the gallery view and couldn’t see clearly what was being signed. We considered sending a Deaf Interpreter to his house in order to provide tactile interpreting, but that was not optimal given the social-distancing measures in place, so we made other arrangements. The person (whether another Deaf participant or the interpreter) was always spotlighted on Zoom, which meant that they were presented in a big screen. Also, all the signing participants in the meeting (CAG members and interpreters) had to wear black and have dark backgrounds so that their hands can be seen more clearly. This made it a much better experience for the Deaf-Blind participant, and he reported that he was able to follow the discussion.
- PLS has hired a Deaf Coordinator who facilitates online meetings. Hiring a Deaf Coordinator made a world of difference for PLS. The Coordinator is able to reach out to all the CAG members directly and ensure their needs are met during the meetings, and that the meeting set up works for them. He is also very well versed in technologies that are suitable for meetings with Deaf, Deaf-Blind and hard of hearing participants, and was the solution provider with Zoom’s spotlight functionality. He was able to host the meeting, ask for clarification when needed, provide additional explanation when needed, and expertly move us through the agenda items. The spotlight functionality also ensured only one person was signing at a time and there was no confusion about who had the floor.
This project needs to move along. One of the reasons there was urgency with how to continue the meetings during these unprecedented times was the sheer fact that this project could not wait because people’s health depended on it. The Coordinator needed to be hired, the Request for Proposals for the service provider had to be finalized, the communications with the Deaf, Deaf-Blind and hard of hearing communities needed to be improved, and medical Sign language interpreting services are an essential service as it enables the provision of healthcare. And as the well-known saying goes: “Where there’s a will (and I would say – need), there’s a way.”







